
🧊 Upside Analysis: Optimizing Athlete Recovery: Evidence-Based Modalities, Market Leaders, and Future Directions

Teams and athletes now have an expanding toolkit for recovery: passive heat (saunas), whole-body cryotherapy and cold-water immersion, compression and pneumatic systems, photobiomodulation / “red-light” (PBM/LLLT), therapeutic lasers (Class 3B / Class 4), and combined cooling/heating systems (contrast therapy, Game Ready style). Each modality has distinct physiological effects (vascular, inflammatory, neuromuscular, mitochondrial), and the best protocol depends on the goal (reduce acute swelling vs accelerate muscle repair vs drive heat adaptation vs improve sleep). The literature is large but not uniform; high-quality meta-analyses and RCTs give useful guidance for selecting modalities and scheduling them relative to training and competition.
Types of recovery protocols
Sauna / Passive heat (Finnish sauna, infrared sauna)
Mechanisms: raises core temperature, increases blood flow, induces heat-shock proteins, may support cardiovascular adaptation and improved tolerance to heat stress. Used for relaxation and chronic adaptation (heat acclimation). (Source: PMC+1)
Cold exposure
Cold-water immersion (CWI / ice baths): vasoconstriction, reduces perceived muscle soreness and some markers of damage; best for short-term symptom relief (24–72 h post high-load sessions). (Source: PubMedPMC)
Whole-body cryotherapy (WBC) / cryostimulation (cryocabin / cryo chambers): very cold air exposures (-100 °C+), anti-inflammatory effects, may improve perceived soreness and sleep in some studies; evidence mixed and protocol-sensitive. (Source: PMCNature)
Contrast therapy / hot–cold cycling
Compression / pneumatic systems (NormaTec, Game Ready, etc.)
Mechanism: intermittent pneumatic compression augments venous return, reduces swelling, and may speed metabolite clearance; often paired with cold or heat. Useful for limb-focused recovery after taxing sessions.
Photobiomodulation / Red-light / Low-Level Laser Therapy (PBM / LLLT)
Mechanism: light in red/near-infrared spectrum stimulates mitochondria (cytochrome c oxidase), reduces inflammation, aids tissue repair, and can reduce delayed-onset muscle soreness (DOMS). Effective in many RCTs, often when applied pre- or immediately post-exercise depending on dose. (Source: PMC+1)
Therapeutic (high-power) Laser therapy (Class 3B / 4)
Used by clinicians for deeper tissue penetration and for accelerating tissue repair/analgesia. Evidence supports efficacy for pain and function in many musculoskeletal conditions, but device parameters (wavelength, power, dose) matter. (Source: PMC)
Cryo-chambers / commercial whole-body cryo
Active recovery & movement / massage / sleep / nutrition
Not modality hardware, but foundational: light movement, sleep hygiene, protein/carbohydrate timing and hydration are critical and often outperform or potentiate hardware interventions. (See recommendations below.)
When to use certain modalities (timing + rationale vs others)
This section is prescriptive: for each common recovery goal, I list recommended modalities and why — and when to avoid them.
A. Immediate post-match (within 0–2 hours): reduce swelling, acute pain, prepare for travel
Best: Cold water immersion (10–15 min at ~10–15 °C) or localized cryotherapy (Game Ready) to reduce soreness and perceived fatigue; compression helps limit swelling. CWI shows benefits for soreness and some performance recovery in the first 24–72 h. (Source: PubMedPMC)
Use caution with: High-dose heat immediately after maximal eccentric load (may blunt adaptive inflammation if the aim is long-term hypertrophy adaptation). Heat can relieve pain but may not be ideal if you want to reinforce adaptation signals.
B. 24–72 h post heavy eccentric or match load: restore neuromuscular function, reduce DOMS
Best: CWI still useful for subjective soreness; PBM / LLLT applied pre- or post-exercise can reduce DOMS and promote recovery of strength in many RCTs; compression sessions (NormaTec) are practical for teams. (Source: PMC+1)
C. Acute injuries or surgery (first days/weeks): reduce swelling, control pain
Best: Cold + compression (Game Ready systems) and clinician-supervised cryotherapy; avoid high-temperature saunas during acute inflammation. Game Ready has clear clinical adoption for post-op rehab.
D. Chronic pain / tissue repair / faster tissue healing (clinician-led)
Best: Therapeutic lasers (Class 3B/4) and PBM with clinician-selected parameters, combined with progressive loading and manual therapy. Laser/PBM show benefits for pain and function and can accelerate healing in some conditions. (Source: PMCMDPI)
E. Sleep, mood, and whole-body recovery (regular routine)
Best: Whole-body cryostimulation (some studies show improved sleep metrics) or regular sauna sessions for cardiovascular/relaxation benefits and possible improved sleep and mood; both may help recovery indirectly. Evidence for WBC improving sleep exists but is mixed; sauna shows cardiovascular and long-term health signals. (Source: PMC+1)
F. Heat adaptation / cardiovascular conditioning (off-season or planned blocks)
Best: Regular sauna bathing (Finnish sauna protocols) to augment heat tolerance, induce HSPs and possible cardiovascular benefits (use in planned blocks, not right before competition). (Source: PMC)
G. When you want circulation + metabolic clearance but minimal systemic stress
Best: Intermittent pneumatic compression (NormaTec) — low risk and easy to deploy on travel days.
Important caveats & interactions (Do not mix blindly)
Cold vs hypertrophy/adaptation: Repeated cold immediately after strength training can blunt anabolic signaling and hypertrophy adaptations. If training priority is long-term strength or hypertrophy, avoid aggressive cold-therapy immediately post-resistance session; reserve it for sessions where immediate recovery is the priority (e.g., tournaments). (See multiple CWI / hot-cold contrast reviews.) (Source: PMCPubMed)
Heat for adaptation: Heat (sauna) can augment endurance adaptations and heat tolerance if used in planned blocks — not within hours of maximal neuromuscular sessions if the goal is recovery for next session. (Source: PMC)
Dose, timing, and individual differences matter: body composition, peripheral fat, prior conditioning, and the exact device parameters (temperature, duration) alter outcomes — personalization is key. (Source: PMCNature)
Stats & Studies (selected high-quality evidence)
(Only a subset—these are representative systematic reviews, RCTs and narrative reviews.)
Cold-water immersion (CWI) meta-analysis: CWI is superior to active recovery and other comparators for reducing muscle soreness and helps neuromuscular recovery up to 24–72 h after team sport exercise. (Systematic review / meta-analysis). (Source: PubMedPMC)
Whole-body cryotherapy (WBC): Mixed results—some RCTs and reviews report reduced soreness and improved inflammation markers; recent studies indicate anti-inflammatory effects (IL-1β down, IL-10 up) but heterogeneity exists in protocol and outcome. Use is promising but not definitive. (Source: NatureFrontiers)
Photobiomodulation / LLLT: Multiple RCTs and systematic reviews show PBM reduces DOMS, improves function and pain, and may enhance muscle recovery when applied with correct dosing and timing. New umbrella reviews support PBM across multiple outcomes. (Source: PMC+1)
Sauna / passive heat: Regular sauna bathing can deliver cardiovascular benefits and improve exercise tolerance; acute sauna after exercise alleviates pain and has some recovery benefits. Evidence ranges from RCTs to observational cohorts (also note rapid recent interest in infrared sauna for longevity). (Source: PMC+1)
Contrast hydrotherapy: Evidence is mixed; CWI generally outperforms contrast for neuromuscular recovery, but contrast can help biochemical markers (CK) and subjective recovery in some contexts. (Source: PubMedPMC)
Key vendors in the recovery space — summary table
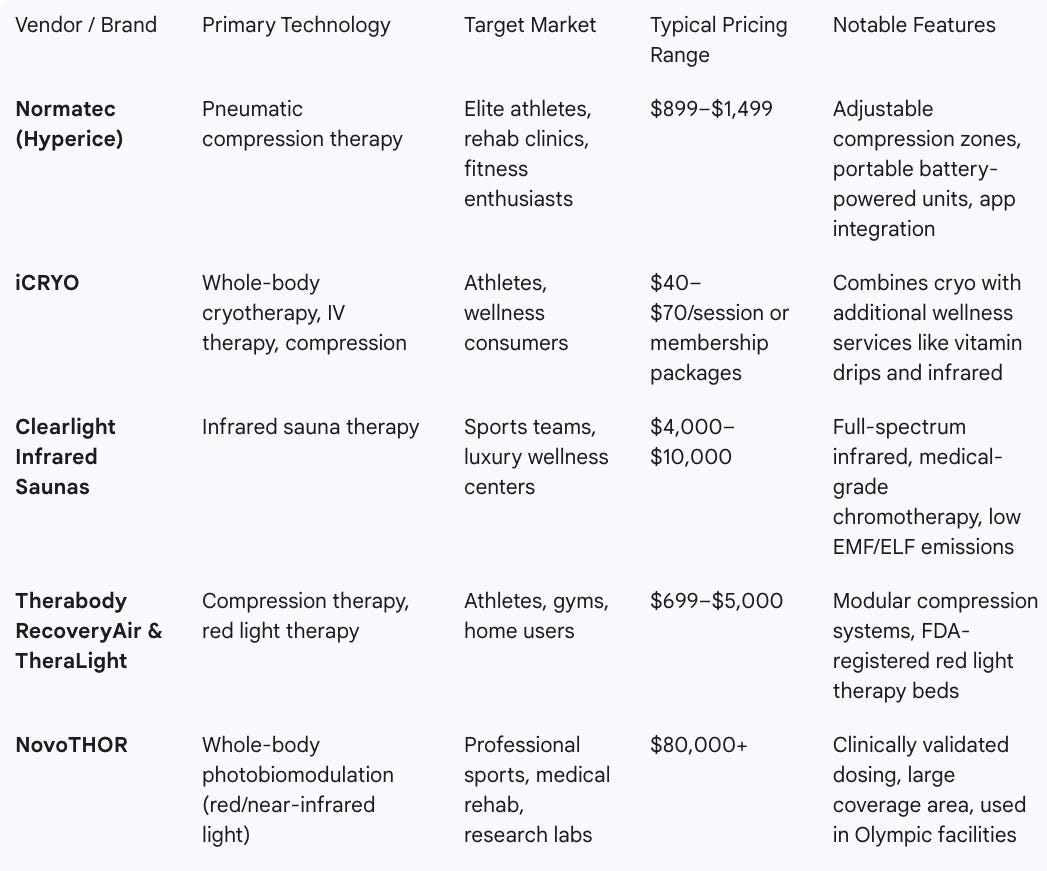

Vendor Summaries
Normatec (Hyperice) – Known for its pneumatic compression sleeves for legs, hips, and arms, Normatec has become a gold standard in recovery rooms of pro teams. Its portability, app integration, and adjustable compression patterns make it ideal for travel and individualized athlete recovery protocols.
iCRYO – A franchise-style recovery service offering whole-body cryotherapy alongside IV vitamin infusions, compression, and infrared sauna options. They appeal to both athletes and the wellness market by packaging multiple modalities under one roof.
Clearlight Infrared Saunas – Specializes in high-end infrared saunas that use full-spectrum wavelengths to target deep tissue recovery, relaxation, and detox. Widely used by pro athletes and luxury wellness spas, they emphasize safety through low EMF/ELF designs.
Therabody RecoveryAir & TheraLight – RecoveryAir focuses on pneumatic compression while TheraLight brings large-format red light therapy beds to the market. Their ecosystem approach allows integration of massage guns, cold therapy, and light therapy into a single brand experience.
NovoTHOR – A premium, research-backed whole-body photobiomodulation device, NovoTHOR is used in Olympic facilities, military rehab centers, and high-performance labs. Its strength is in delivering clinically precise dosing over the entire body in under 20 minutes.
Game Ready – Combines active cold therapy with compression in a portable device, ideal for post-injury and post-surgical recovery. Common in sports medicine and physical therapy clinics, it’s praised for speeding recovery while reducing swelling.
CryoBuilt – Manufactures electric whole-body cryotherapy chambers that remove the need for liquid nitrogen, making them safer and more consistent in temperature control. They offer custom branding and designs tailored to pro team facilities.
LightStim – Offers a wide range of FDA-cleared LED light therapy devices from small handheld units to full-body beds. Known for durability and wavelength versatility, they cater to both professional trainers and home users.
Future of recovery modalities
Personalized dosing and periodization: recovery prescriptions (modality, dose, timing) will be individualized using load monitoring (GPS, HRV, biochemical markers) and adapted based on athlete response. Expect decision-support software to recommend modality choice based on objective load and goals.
Hybrid systems: combined devices that can deliver targeted PBM + localized cooling/compression in a single session.
Better evidence stratification: larger multi-site RCTs and umbrella meta-analyses (ongoing) will refine which modalities work for which athlete types and sport demands (team vs individual, endurance vs strength). Recent umbrella reviews cover PBM and other modalities, improving evidence clarity. (Source: PMC+1)
Wearable feedback loops: integration of sleep, HRV and wearable biomarkers to time interventions (e.g., cryotherapy when HRV drops; sauna when sleep metrics are poor).
Lower cost clinical lasers / home PBM: more accessible devices with validated dosing for teams and clinics.
Practical recommendations to teams
Make goals explicit — define whether you are prioritizing (A) immediate symptom relief to get players ready the next day, (B) long-term adaptation (hypertrophy/endurance), or (C) post-injury clinical recovery. Modality choice depends on this.
Periodize heat and cold — avoid routine CWI after heavy resistance sessions aimed at hypertrophy (it blunts anabolic signaling); use heat (sauna) in planned adaptation blocks for endurance and heat tolerance. (Source: PMC+1)
Use compression and PBM as low-risk daily tools — Normatec / compression boots and Joovv PBM panels are practical for daily deployment in team rooms and have favorable safety profiles.
Safety and medical oversight — WBC and extreme cold exposures carry cardiovascular risks for some athletes. Screen cardiovascular history and have protocols in place; keep clinicians in the loop. (Source: Nature)
Cost-effectiveness & logistics — for many teams: start with compression boots + a PBM panel + access to rented Game Ready units for acute injury; consider sauna installation if you have space and a long-term plan for heat adaptation. Cryo chambers often require heavy capital and operating costs and are best for clubs with high utilization or revenue models.
Measure outcomes — track subjective soreness, readiness (questionnaire), jump power, and objective load (GPS/IMU) and pair interventions with these metrics so the team learns what works for their athletes.
Conclusion
There is no single “best” recovery tool — each modality has strengths and limitations. The evidence supports cold (CWI) and compression for short-term symptom relief, PBM/LLLT for reducing DOMS and aiding tissue repair (when dosed correctly), and sauna for cardiovascular and heat-adaptation benefits. Whole-body cryotherapy shows promise for soreness and sleep in some studies but remains heterogeneous in evidence and logistics. Teams should align modality selection to the recovery goal, periodize interventions to avoid blunting long-term adaptations, and integrate low-risk, high-utility tools (compression, PBM) early. Finally, vendor choice should reflect budget, space, clinical oversight, and expected utilization.
You may also like:

Love seeing recovery framed with actual evidence — because the hype around ice baths is usually all “burn fat fast!” while the real benefits are so much deeper. Cold exposure isn’t about torching calories (studies show fat mass barely changes) — it’s about activating brown fat, lowering inflammation, and rewiring hormones in ways athletes and everyday people can use.
I just wrote about the science (plus my own snow-pile fail 🤦♀️) here:
👉 https://leareset.substack.com/p/if-cold-plunging-for-fat-loss-feels
Sometimes the smartest recovery tool isn’t what the scale shows, but what your cells are quietly doing in the background.