
⭐Upside Studies: Factors Important to Patient Decision-Making After Ulnar Collateral Ligament Injury in Competitive High School and Collegiate Baseball Players

Title: “Factors Important to Patient Decision-Making After Ulnar Collateral Ligament Injury in Competitive High School and Collegiate Baseball Players”.
Authors:
a) Elise C. Bixby,† MD, Rifat Ahmed, †
b) MS, Kira Skaggs, † MD, Hasani W. Swindell, † MD,
c) Thomas A. Fortney, † MD, and Christopher S. Ahmad,* † MD
Investigation performed at the Department of Orthopedic Surgery, Columbia University Irving Medical Center, New York, New York, USA
Background: Patients are faced with several treatment decisions after an ulnar collateral ligament (UCL) injury: nonoperative versus operative treatment, repair versus reconstruction, and immediate versus delayed surgery.
Purpose/Hypothesis: The aim of this study was to investigate the factors important to patients when deciding which treatment to pursue after a UCL injury. We hypothesized that (1) length of time away from sports and seasonal timing would be important to patients and (2) treatment decision-making would be heavily influenced by how many and which seasons of their baseball career would be missed.
Study Design: Cross-sectional study.
Methods: High school and collegiate baseball players with UCL tears treated at an academic institution were surveyed retrospectively on their sports participation at the time of injury and their UCL injury treatment decisions. Respondents rated the influence of various factors on a 5-point Likert scale, and they selected the top 3 factors and the single most important factor influencing their treatment decisions. Multiple logistic regression analysis was used to assess the relationship between player characteristics and factors important to their treatment decision.
Results: A total of 83 athletes completed the survey; 40 were in high school and 43 were in college at the time of injury; 7 were treated nonoperatively and 76 underwent surgery (66 immediately and 10 in a delayed fashion), 10 with UCL repair and 66 with UCL reconstruction.
The ability to play competitive baseball in the long term was very important or extremely important to 90% of players, while the ability to play in the short term was very important or extremely important to 17%. Length of recovery and seasonal timing were also important factors for 53% and 54% of players, respectively, and almost all (90%) highly valued advice from a surgeon. Possible failure of nonoperative treatment leading to increased time away and the possible loss of 2 consecutive baseball seasons heavily influenced decision-making in 41% of respondents.
Conclusion: Survey respondents were driven by the desire to play baseball in the long term. Treatment decisions were influenced by the length of recovery and by the seasonal timing of their injury, both of which affect how many and which seasons of baseball a player may miss. Patients found advice from their surgeon to be extremely important to decision-making.
Keywords: patient preferences; return to play; seasonal timing; UCL reconstruction; UCL repair; ulnar collateral ligament injury.
The ulnar collateral ligament (UCL) is an important medial stabilizer of the elbow, particularly for overhead athletes.8,11 The valgus force generated by throwing, especially a baseball or javelin, or by upper extremity weight bearing in wrestling or gymnastics, can lead to degenerative changes or acute injury to the UCL. While UCL injuries typically do not impact activities of daily living, they can cause significant pain and dysfunction for athletes who continue to participate in their sport. 8,11
Historically, UCL injuries were seen as career-ending for baseball players.10,14 However, there have been significant advances in both nonoperative and operative treatments, such that the majority of athletes can return to play (RTP). 1,6,9,13 Nonoperative treatments now include improved rehabilitation programs and platelet-rich plasma injections, while operative treatments include either UCL repair or UCL reconstruction. 5 Indications for operative fixation include a failure of nonoperative treatments or an acute complete UCL tear on magnetic resonance imaging. 7- 9,14 Patients without degenerative changes to the UCL are candidates for UCL repair, with proximal tears having better outcome than midsubstance tears. 7,8,16 The UCL can be reconstructed regardless of the quality of the native UCL tissue, using a number of different methods. 10

Thus, nonoperative treatment, UCL reconstruction, and/or UCL repair may be options for some patients, depending on the characteristics of their UCL injury. How- ever, the different treatment options vary in terms of RTP rates and in the average length of time for a patient to RTP or to competition. 1,4,6,7
For baseball pitchers, RTP after nonoperative treatment can take as long as 4 months. RTP after UCL repair ranges from 6 to 8 months and from 12 to 14 months after UCL reconstruction. 1,4,6 Many patients who injure their UCL have a desire to continue playing baseball. Failure of a trial of nonoperative treatment can adversely affect a player’s ability to extend their careers if they miss multiple seasons (seasonal timing) or miss an important season for recruitment to the next level of play (career timing). Understanding how seasonal and career factors are considered in the decision-making process is critical to clinicians, so they can fully discuss the implications of different treatment options and tailor recommendations accordingly.
The aim of this study was to investigate which factors are important to patients in deciding what treatment to pursue after a UCL injury. We hypothesized that (1) factors related to the length of time away from sport, seasonal timing, and career timing would be important to patients; and (2) patient decision-making would be heavily influenced by how many, and which, seasons of baseball a player would miss as a result of postoperative rehabilitation.
METHODS
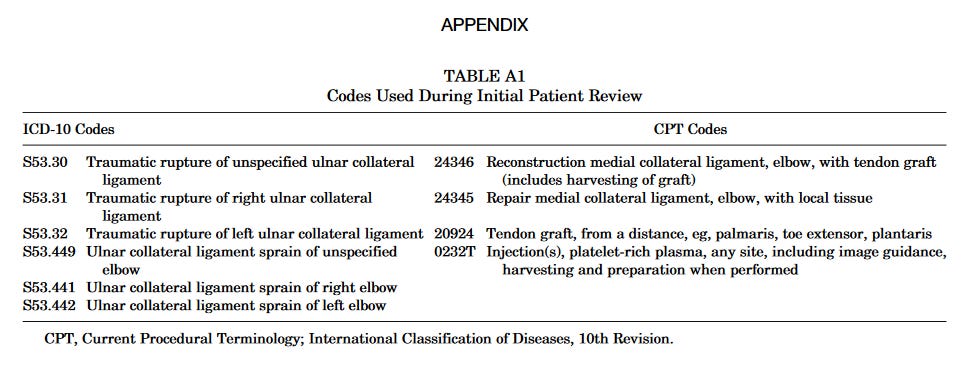
After obtaining institution institutional review board approval, we queried the patient records for both International Classification of Diseases, 10th Revision and Current Procedural Terminology codes related to UCL injury, UCL repair, and UCL reconstruction at a large urban academic institution from January 1, 2018, through December 31, 2021. The full list of codes utilized is available in Appendix Table A1. This list was then screened for duplicate patients. Clinic notes for each patient were screened to confirm that the patient played high school or college baseball at the time of injury and that the patient was diagnosed with a UCL tear by an attending surgeon. Injuries noted to be UCL “sprains” or “strains” were excluded, as were UCL tears in the setting of an elbow dislocation.

Patients with and without concomitant ulnar neuritis were included. While the initial query included patients seen by multiple surgeons, all patients who met inclusion criteria were under the care of a single sports medicine fellowship-trained orthopaedic surgeon. Patients and/or their parents were contacted via telephone and/or email, and those agreeing to participate in the study were sent a survey via Qualtrics. The survey is available separately as Supplemental Material.

The survey instrument consisted of 5 sections. The first section presented the study goals and obtained patient or parental consent. The remainder of the study was completed by the patient. The second section collected patient demographics, while the third section collected information about sports participation. The fourth section was comprised of the Athletic Identity Measure Survey (AIMS), which quantifies how integral a patient’s role as an athlete is to their identity. The final section asked questions specific to treatment decision-making. The patient was asked what treatment option they chose (nonoperative, UCL repair, or UCL reconstruction; definitive treatment shortly after diagnosis or in a delayed fashion) and how important different factors were to their decision-making. Each factor was first rated on a 5-point Likert scale ranging from “not at all important” to “extremely important.” Patients were then asked to select the 3 factors that were most important to their decision-making, then asked to select the single most important factor from this subset. Lastly, patients were asked about how the risk of missing 1 versus 2 seasons of baseball or missing specific seasons (eg, junior year of high school) impacted their treatment decision-making.

Survey data were exported from Qualtrics, and data analysis was conducted using IBM SPSS Statistics (Version 25). Demographic characteristics, including age and AIMS score, were calculated as means ± standard deviations, and specific response rates to survey questions were calculated as percentages. Multiple logistic regressions were used to assess the relationship between player characteristics and factors important to their treatment decision. Significance was set at P < .05
RESULTS
UCL tears were identified in 295 high school or college baseball players, and 184 were able to be contacted over the phone or by email.
A total of 176 patients agreed to participate, and 83 patients completed the survey (Figure 1), on average 1.5 ± 1.2 years after their UCL injury. Demographics at the time of injury are listed in Table 1. Respondents were, on average 18.8 ± 2.0 years old at the time of injury, and all (100%) were male. A total of 40 patients were in high school and 43 were in college when they sustained their UCL injury.

The majority (93%; n ¼ 77) played baseball exclusively. Other sports played included basketball (n ¼ 4; 5%), golf (n ¼ 1; 1%), and football (n ¼ 1; 1%).
Respondents had an average AIMS score of 54 ± 10 out of 70; 36% (n ¼ 30) of patients were injured in the preseason, 17% (n ¼ 14) early in the season, 8% (n ¼ 7) in midseason, 23% (n ¼ 19) late in the season, and 16% (n ¼ 13) in the off-season.
Of all survey respondents, 7 were treated nonoperatively, 66 underwent surgery as soon as possible after receiving their diagnosis, and 10 underwent surgery in a delayed fashion. Of those undergoing surgery, 10 had a UCL repair with an internal brace and 66 had a UCL reconstruction. Of those receiving a UCL reconstruction, 6 respondents had discussed undergoing a UCL repair preoperatively, but their UCL was deemed irreparable intraoperatively.
Of those who elected a UCL reconstruction, 51% stated a UCL repair was not an option based on the characteristics of their UCL tear, while 49% thought that a reconstruction would be “stronger or more reliable in the long run” as compared with a UCL repair. Of those who elected for UCL repair, including those ultimately receiving a UCL reconstruction because of an irreparable UCL despite initially preferring a repair, 69% (n ¼ 11) did so because they thought it would allow them to return to playing baseball faster than would a reconstruction.
Factors impacting patient decision-making are presented in Table 2 and Figure 2. Among high school players whose treatment decision impacted whether they could play baseball their junior year (n ¼ 17), 29% said it was a very important factor in their decision-making while an additional 29% said it was the most important factor in their decision-making. Of high school respondents whose treatment decision impacted whether they could play their senior year of baseball (n ¼ 31), 39% said it was a very important factor and 26% said it was the most important factor in their decision-making. When respondents would miss 1 versus 2 seasons of high school baseball, depending on their treatment chosen (n ¼ 61), 28% stated this weighed heavily in their decision and 13% said this was the most important factor in their decision-making.

Based on logistic regression, the importance of seasonal timing to a patient was not significantly influenced by the degree to which they identify as an athlete (as quantified by an AIMS score), their year in high school or college, or their plans to play baseball in college or professionally. Similarly, neither consideration or concern for the length of recovery nor the time away from sports were influenced by these factors. The importance of being able to play baseball in the short term was associated only with the patient’s AIMS score.

With each 1-point increase in AIMS score, the odds of a patient reporting the ability to play in the short term as “very important” or “extremely important” increased by a factor of 1.146 (95% CI, 1.005-1.307; P ¼ .042).
There was no significant association between the degree to which a respondent identified as an athlete (as quantified by an AIMS score), their year in high school or college or their plans to play baseball in college or professionally and their treatment decision (nonoperative versus operative treatment and immediate vs delayed surgery).
Similarly, there was no significant association between the importance of each factor to a patient and whether they chose nonoperative or operative treatment.
However, when patients chose to undergo surgery, they were affected by several factors. Players who rated the ability to play baseball in the long term as “very” or “extremely important” were much less likely to delay surgery as compared with players who rated this factor as less important (odds ratio [OR] ¼ 0.018, P ¼ .001). Similarly, those that rated the length of recovery as “very” or “extremely important” important were less likely to delay surgery (OR ¼ 0.048, P ¼ .008).
However, those who rated time away from sports as “very” or “extremely important” important were more likely to delay surgery (OR ¼ 15.591, P ¼ .014).
DISCUSSION
The results of this study indicated that patient decision-making is driven by pain/discomfort while throwing and the ability to play baseball in the long term, with a respective 89% and 90% of patients reporting these factors as very important or extremely important.
Length of recovery and seasonal timing were also important components to patient decision-making and are in the top 3 factors affecting decision-making for 37% and 36% of patients, respectively.
Advice from a surgeon weighed heavily in the decision and was very or extremely important to 90% of respondents. Athletes, specifically baseball players, are presented with several treatment decisions when they receive a diagnosis of a UCL injury.

Depending on characteristics of the injury, UCL repair or reconstruction may be considered. Nonoperative treatments are always an option, although they may not have acceptable outcomes for players with complete tears wanting to return to competitive play. 1
Patients also can choose to have surgery imminently after diagnosis or to delay surgery until a time that is more convenient, based on their season of play and other life events.
To our knowledge, this is the first study that evaluated for factors that influence patient decision-making following a diagnosis of a UCL tear.
Return to Play
This study included a cohort of predominately single-sport baseball players with strong athletic identities. They played competitively across a spectrum of levels, including high school and college teams. The majority of high school patients planned to play in college and a significant number of patients injured during college aspired to play professionally (Table 1).
Accordingly, 90% of patients felt that the ability to play competitive baseball in the long term was “very important” or “extremely important” to their treatment decision-making.
It was a top-rated factor, in terms of importance, for over half of respondents and rated as the most important factor for over one-third of respondents

Patients want to return to baseball, and nonoperative treatments, UCL repairs, and UCL reconstructions can all result in high rates of RTP. 1,4,5,6,7
However, RTP rates for each treatment option are significantly impacted by tear characteristics. RTP rates range from 66% to 100% for partial proximal UCL tears treated nonoperatively with platelet-rich plasma and/or rehabilitation, but high-grade tears and distal tears tend to do poorly.
5 RTP rates are between 92% and 97% for UCL repair with modern techniques such as suture augmentation or the use of an internal brace, in patients with proximal tears and good tissue quality of the UCL. 2,6,13,15,16 In contrast, results after UCL reconstructions are not limited by tear pattern or tissue quality. UCL reconstructions had an 85.7% ± 8.5% rate of return-to-competition at the preinjury level or higher in a meta-analysis by Anderson et al.1
Historically, a trial of nonoperative treatment was considered the gold-standard for all patients. 3,7-9,14 However, more recent literature on appropriate patient selection has helped surgeons better direct patients toward treatment options that are likely to allow patients to RTP, often bypassing nonoperative treatment for complete or distal tears. 5,8 Tear patterns were not assessed explicitly in this study but are considered routinely during patient counselling and shared decision-making at our institution.
Interestingly, there was no significant correlation in this study between how important playing baseball in the long term was to a patient and their choice of operative or nonoperative treatment.

This may be a statistical limitation, in that the large majority of patients chose operative treatments and that almost all patients felt playing baseball in the long term was “very” or “extremely important” to decision- making. Alternatively, it may reflect that patients are being counselled predominantly on the treatment options that have high RTP rates for their specific tear pattern, given the overwhelming importance of RTP to most of these patients.
Length of Recovery
Length of recovery and time away from baseball were “very” or “extremely important” to a large number of respondents: 53% and 45%, respectively. In addition, of patients who elected a UCL repair, 69% did so because they thought it would allow them to return to baseball faster than a reconstruction.
Indeed, the anticipated length of recovery depends on the procedure. Position players typically return to play at around 6 months after a UCL repair, 6,7,13,17 as compared with 9 to 12 months after a UCL reconstruction. 1,12
The anticipated length of recovery also depends on whether the patient is a pitcher and wants to return to pitching.
Pitchers return around 12 to 14 months versus 9 to 11 months for position players after UCL reconstruction. 1,4 This discrepancy in length of rehabilitation seems to be smaller after UCL repairs.

Pitchers returned at on average 7.3 months versus 7.1 months for position players after UCL repair in a study by Dugas et al.6 Being a pitcher rather than a position player was “very” or “extremely important” in the decision-making of 68% of respondents in this study. Pitchers were not differentiated from position players, so it is not possible to determine what percentage of pitchers this represents and what percentage of pitchers would consider transitioning to a position player to RTP earlier.
These preferences need to be discussed with patients so that the appropriate lengths and benchmarks of rehabilitation protocols can be factored into decision- making. Beyond expectation setting, understanding the different lengths of recovery may influence a patient’s decision between reconstruction and repair, if both are viable options for their UCL tear.
Seasonal Timing
The timing of recovery was also found to be important to patients in our investigation. Specifically, seasonal timing as “very” or “extremely important” to 54% of respondents and was 1 of the top 3 factors influencing treatment decision-making for over one-third of patients in this cohort (Table 1 and Figure 2).
Seasonal timing refers to when in the season (eg, preseason, midseason, late season, etc) an injury and/or recovery occurs, and how that impacts the player’s ability to participate in the current and subsequent seasons of their sports career. As previously discussed, the length of rehabilitation depends on whether a UCL repair or reconstruction is performed and whether the patient is a pitcher or position player. However, length of recovery does not equate directly to time away from sports. Seasonal timing needs to be taken into account.
An extra 4 months of recovery for a UCL reconstruction instead of a repair may take place during the off-season or delaying surgery by 4 months may allow a player to return at the end of the off-season rather than at the beginning. No additional competitive play is missed.
However, there are a number of cases in which the seasonal timing of the injury and the treatment chosen do impact how much of or how many seasons a player misses.

As an example, a player injured in May is approximately 8 months away from the next season, beginning in February. This patient will miss the season when the injury occurred with 3 to 4 months of nonoperative treatment. If nonoperative treatment fails and he requires surgery, he will miss the subsequent season - 2 seasons altogether.
Alternatively, if that patient undergoes UCL repair shortly after injury, he can recover in time for the upcoming season. The impact of seasonal timing, as highlighted in this example, appears to play a significant role in treatment decision- making for some patients. Indeed, missing 1 versus 2 sea- sons of baseball heavily influenced decision-making for 41% of respondents in this study.
Career timing also appears to be important, in that the particular season a player misses within their career also influences their decision-making. Playing the junior and senior seasons of baseball in high school seem important to many patients. Junior year in high school is often a recruitment period. Some players are focused on not only the ability to play in college but on scholarship funding.
Senior players are often motivated to RTP because it may be their year of best performance at the high school level. It is typically the last year to play with their current team of friends and coaches.
A total of 58% of players in the study indicated the ability to play their junior year was very important or the most important factor influencing when to have surgery and what type of surgery to have. Similarly, 65% said whether they could play their senior year was very important or the most important factor.
However, this did not seem to be associated directly with a need or desire to participate in recruitment events. Only 17% of respondents felt that their decision was influenced significantly by the ability to play baseball in the short term for recruitment purposes (for example, for a showcase game) and only 2% felt that this was the most important factor in their decision-making.

This is despite the high rates of patients planning to play college and/or professional baseball. The importance of being able to play in the short term, however, was positively correlated with a patient’s AIMS score, that is, the intensity of their athletic identity. It is possible that the seasonal timing of the injuries in this cohort did not put them at risk for missing recruitment events or that they had other pathways to continue to play baseball in college.
Players with strong athletic identities may also value their high school baseball seasons not just as part of the pathway to college or professional careers, but for the psychologic and social benefits of playing in these formative years.
Role of the Surgeon
Within the cohort studied, patients were found to value the opinions and perspectives of their surgeon. Advice from a surgeon was very or extremely important for 90% of respondents, a top 3 factor for 49% of respondents and the most important factor for 19% of respondents.

In comparison, input from family and friends was a top factor for only 11%, and input from someone with a previous UCL injury was a top 3 factor for only 8%. Input from a coach or trainer was very or extremely important for about one-third of players but none listed it in the top 3 most important factors influencing their decision-making.
Surgeons, however, play a significant role in presenting and interpreting the literature on RTP and failure rates of different tear patterns and treatment options. Surgeons also typically facilitate the rehabilitation process and clearance for RTP, with significant variation in protocols between clinicians. 1 Patients need to understand what their specific recovery would entail after different treatment options with their specific surgeon.
Equally importantly, surgeons can help elicit what factors are most important to the patient - for example, how important it is to return as a pitcher rather than a position player or how important it is for them to finish out their senior high school baseball season versus be ready for the preseason as a freshman in college. Incorporating these factors, a surgeon can guide the patient to a treatment decision that best fits the patient’s individual circumstances. Patients often come to a specific surgeon based on their reputation, but it is these tailored, nuanced discussions which build rapport and confidence in what is ultimately a shared decision between patient and surgeon and often parents and coaches as well.
Limitations
There are a number of limitations to this study that warrant mention. The relatively low survey response rate (45% of those contacted and 28% of those identified) puts the study at risk for selective nonresponse biases.
However, it is the first of its kind to assess patient perspectives on treatment decision-making in this context. As with all retrospective studies, it is also at risk for recall bias. The participants did represent a wide range of ages of competitive baseball players, from high school freshman to senior collegiate athletes, but there was a predominance of players treated operatively. Furthermore, pitchers were not differentiated from position players, though implications for both have been discussed. UCL tear characteristics (eg, tear location or tissue quality on MRI) were not assessed in this study, as it focuses on patients’ conceptualization of their injuries and treatment options, rather than on the injuries themselves. There may also be some overlap in how patients conceptualize different factors (eg, time away from sports and length of recovery), which may have minimized the influence of the individual factors. Finally, this study focused on the decision-making process itself, and did not assess a patient’s satisfaction with their decision or decision regret.
CONCLUSION
In conclusion, this study is the first to evaluate factors that influence patient decision-making after UCL injuries. Our findings suggest that high school and collegiate baseball players are driven by the desire to play baseball in the long term. Their treatment decision appears to be influenced by the length of recovery of different treatment options and by the seasonal timing of their injury, both of which affect how many and which seasons of baseball a player may miss out on. Above all, patients find advice from their surgeon extremely important to their decision-making. Surgeons must be cognizant of factors influential to patient decision-making after a UCL injury, so as to provide contextualized advice on which treatment and timing may be most appropriate for the individual athlete.
ACKNOWLEDGMENT
The authors acknowledge Prakash Gorroochurn, PhD, for his assistance with statistical analyses for this study.
Supplemental material for this article is available at https://journals.sagepub.com/doi/full/10.1177/ 23259671231183486#supplementary-materials
REFERENCES
1. Anderson MJJ, Crockatt WK, Mueller JD, et al. Return-to-competition criteria after ulnar collateral ligament reconstruction: a systematic review and meta-analysis. Am J Sports Med. 2022;50(4):1157-1165.
2. Argo D, Trenhaile SW, Savoie FH, Field LD. Operative treatment of ulnar collateral ligament insufficiency of the elbow in female athletes. Am J Sports Med. 2006;34(3):431-437.
3. Bogdanov JM, Bolia IK, Benvegnu N, Michener LA, Weber AE, Petrigliano FA. Rehabilitation following ulnar collateral ligament reconstruction in overhead-throwing athletes. JBJS Rev. 2021;9(4):e20.00154.
4. Camp CL, Conte S, D’Angelo J, Fealy SA. Following ulnar collateral ligament reconstruction, professional baseball position players return to play faster than pitchers, but catchers return less frequently. J Shoulder Elbow Surg. 2018;27(6):1078-1085.
5. Cascia N, Uhl TL, Hettrich CM. Return to play following nonoperative treatment of partial ulnar collateral ligament injuries in professional baseball players: a critically appraised topic. J Sport Rehabil. 2019; 28(6):660-664.
6. Dugas JR, Looze CA, Capogna B, et al. Ulnar collateral ligament repair with collagen-dipped fibertape augmentation in overhead- throwing athletes. Am J Sports Med. 2019;47(5):1096-1102.
7. Erickson BJ, Bach BR, Verma NN, Bush-Joseph CA, Romeo AA.Treatment of ulnar collateral ligament tears of the elbow: is repair a viable option? Orthop J Sports Med. 2017;5(1):2325967116682211.
8. Erickson BJ, Harris JD, Chalmers PN, et al. Ulnar collateral ligament reconstruction: anatomy, indications, techniques, and outcomes. Sports Health. 2015;7(6):511-517.
9. Erickson BJ, Romeo AA. The ulnar collateral ligament injury: evaluation and treatment. J Bone Joint Surg Am. 2017;99(1):76-86.
10. Jensen AR, LaPrade MD, Turner TW, Dines JS, Camp CL. The history and evolution of elbow medial ulnar collateral ligament reconstruction: from Tommy John to 2020. Curr Rev Musculoskelet Med. 2020; 13(3):349-360.
11. Loftice J, Fleisig GS, Zheng N, Andrews JR. Biomechanics of the elbow in sports. Clin Sports Med. 2004;23(4):519-530,vii-viii.
12. Moore AR, Fleisig GS, Dugas JR. Ulnar collateral ligament repair. Orthop Clin North Am. 2019;50(3):383-389.
13. O’Connell R, Hoof M, Heffernan J, O’Brien M, Savoie F. Medial ulnar collateral ligament repair with internal brace augmentation: results in 40 consecutive patients. Orthop J Sports Med. 2021;9(7): 23259671211014230.
14. Rossy WH, Oh LS. Pitcher’s elbow: medial elbow pain in the overhead-throwing athlete. Curr Rev Musculoskelet Med. 2016;9(2): 207-214.
15. Savoie FH, Trenhaile SW, Roberts J, Field LD, Ramsey JR. Primary repair of ulnar collateral ligament injuries of the elbow in young athletes: a case series of injuries to the proximal and distal ends of the ligament. Am J Sports Med. 2008;36(6):1066-1072.
16. Torres SJ, Limpisvasti O. Ulnar collateral ligament repair of the elbow-biomechanics, indications, and outcomes. Curr Rev Musculoskelet Med. 2021;14(2):168-173.
17. Walters BL, Cain EL, Emblom BA, Frantz JT, Dugas JR. Ulnar collateral ligament repair with internal brace augmentation: a novel UCL repair technique in the young adolescent athlete.
You may also like:
⭐⚽ Upside League Profile: Brazilian National Soccer Team & Chat with Guilherme Passos, Sports Scientist On His Favorite Technologies, The Best Players/Coaches He Worked With.
🔥 Upside Chat: Dave Hancock, CEO, Apollo (Leading Athlete Management Systems (AMS) vendor)
🔥Upside Chat: Alexi Pianosi, Strengths and Conditioning Coach, Pittsburgh Penguins (NHL)
🔥Upside Chat: Pierre Barrieu, High Performance Director, Toronto FC (MLS)
🔮 2022 Upside Top Sports Tech Predictions (NFT/Metaverse, Sports Performance, IPOs/M&As..)